
Most healthcare practices think they're compliant because they bought a secure EHR, gave staff a policy binder, and had someone sign a few forms. That's not a compliance program. That's a loose collection of tasks.
The question is simpler and tougher. If a regulator asked for risk analysis records, access logs, vendor agreements, training evidence, and breach procedures tomorrow, could the practice produce them quickly and confidently? If the answer is no, the practice isn't operating with reliable HIPAA compliance for healthcare. It's operating on hope.
Table of Contents
- Is Your Practice Truly HIPAA Compliant
- Establish Your HIPAA Compliance Foundation
- Conduct an Actionable HIPAA Risk Assessment
- Create Essential Policies and Manage Vendors
- Build Your Breach Response and Notification Plan
- Maintain Compliance Through Monitoring and Audits
- Frequently Asked Questions About HIPAA Compliance
Is Your Practice Truly HIPAA Compliant
A practice doesn't need a major cyberattack to end up in trouble. Most compliance failures come from ordinary operational mistakes, weak follow-through, and missing documentation.
The enforcement record makes that plain. Since the HIPAA Privacy Rule's compliance date, the HHS Office for Civil Rights has received over 374,321 HIPAA complaints, leading to 152 cases with settlements or penalties totaling over $144 million. The same record also shows that accidental negligence is twice as likely as malicious attacks, which puts staff mistakes and process gaps at the center of the problem, not just hackers or advanced threats, as summarized in these HIPAA violation statistics.
That should change how a practice owner thinks about HIPAA compliance for healthcare. Compliance isn't a legal side project. It's basic operational discipline. A misdirected email, an old laptop that wasn't wiped, or a shared login that nobody shut off can create the same kind of exposure that owners usually associate with a breach headline.
Compliance works best when a practice treats it like infection control. It's built into daily behavior, not pulled off a shelf when someone asks.
A better approach is to stop asking, “Are the boxes checked?” and start asking, “Can the practice prove control over patient data every day?” That means documented safeguards, regular review, and clear accountability, even if the practice doesn't have a full-time compliance officer.
For clinics that need a practical starting point, reviewing what a modern HIPAA-compliant IT services approach looks like helps clarify the difference between scattered security efforts and a working compliance framework.
Establish Your HIPAA Compliance Foundation
HIPAA gets overcomplicated because practices hear legal terms and assume they need a giant enterprise program. They don't. They need a disciplined one.
At the core, HIPAA compliance for healthcare rests on three safeguard categories. Each one answers a different question. Who is allowed to do what? Where is sensitive information physically exposed? What technology controls enforce the rules?
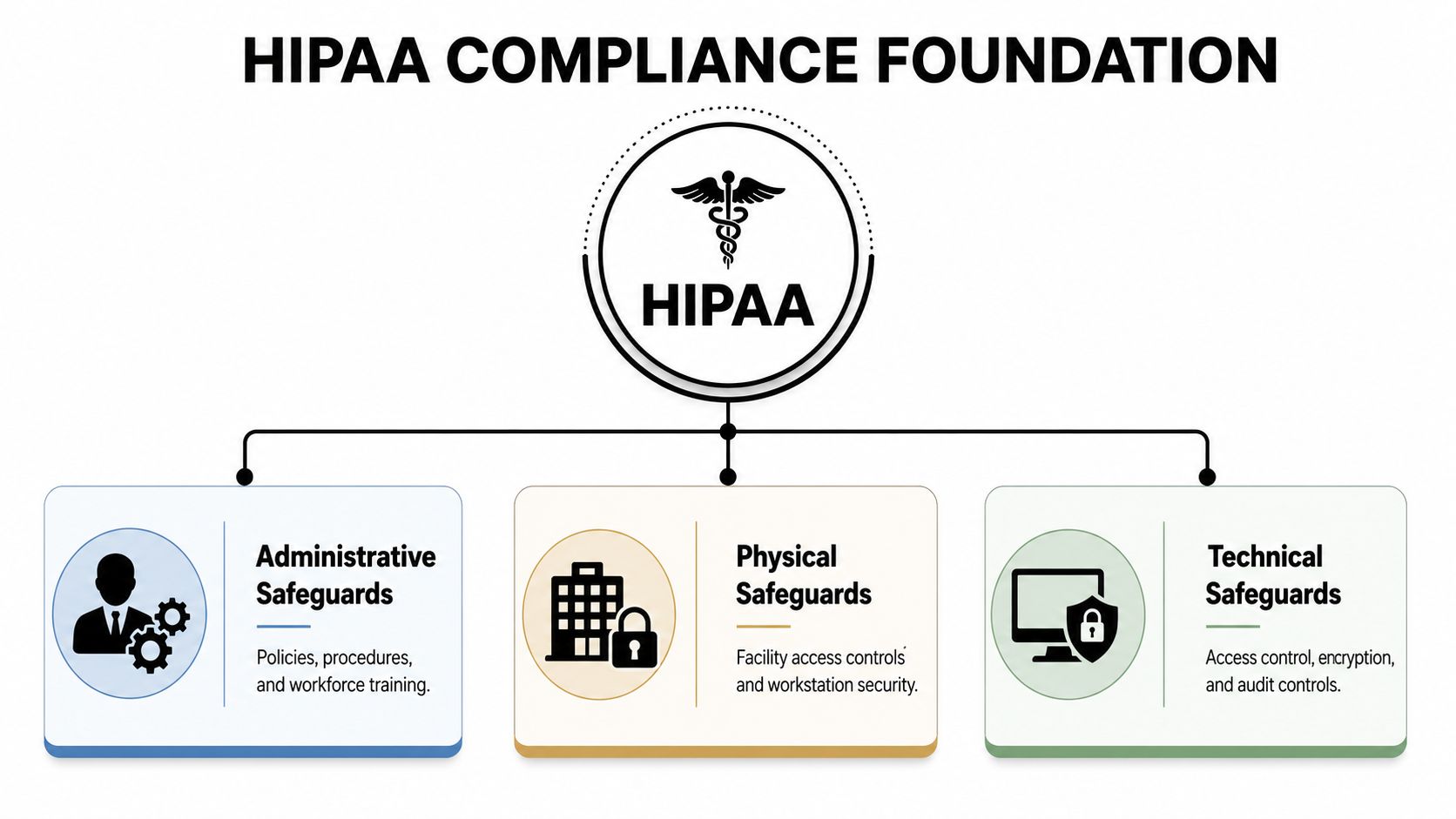
Know what each safeguard actually does
Administrative safeguards govern decisions and behavior. They include policies, procedures, assigned responsibilities, training, and access decisions. If a receptionist can view more records than the role requires, that's an administrative failure before it becomes a technical one.
Physical safeguards protect the spaces and devices that hold or reach patient data. Server closets, front-desk screens, exam room workstations, printers, shredding bins, and retired laptops all belong here. Many practices ignore physical exposure because it feels old-fashioned. That's a mistake.
Technical safeguards enforce protection through systems. Access control, encryption, audit logs, endpoint protection, and authentication sit in this layer. A successful HIPAA security program depends on compliance analyses, policy development, and workforce training, and one commonly missed technical requirement is audit controls that log exactly who accessed and altered electronic PHI, including the date, time, and specific action taken, as outlined in this HIPAA security best practices discussion.
A practice that wants cleaner records should also think about workflow design, because bad workflows often create compliance shortcuts. A useful example is this guide on clinical documentation workflows, which shows how documentation processes can either reduce friction or push staff toward risky workarounds.
Treat the safeguards as one operating system
These categories aren't separate checklists. They work together.
| Safeguard | What it controls | Common clinic example |
|---|---|---|
| Administrative | Staff decisions and approved processes | Role-based access, training, sanctions |
| Physical | Rooms, devices, media, and visible exposure | Locked offices, screen placement, secure disposal |
| Technical | System-enforced protections | Encryption, logging, authentication |
A practice usually fails at the handoff points. Staff are trained, but access isn't updated. Devices are encrypted, but old backups aren't controlled. A vendor is approved, but nobody confirms how access is logged.
Practical rule: If a safeguard depends on memory alone, it isn't stable enough.
That's why the foundation should be built like an operating routine, not a compliance binder. Every control needs an owner, a review point, and evidence that it's working.
Conduct an Actionable HIPAA Risk Assessment
A risk assessment shouldn't be treated like annual paperwork. It's the practice's way of discovering where patient data can be exposed before someone else discovers it first.
Too many clinics start with a template and fill in generic answers. That creates a false sense of security. A useful risk assessment begins with the actual environment, not a prewritten spreadsheet.
Start with where PHI actually lives
Patient data doesn't stay neatly inside one application. It lives in email attachments, scan folders, billing exports, remote laptops, archived drives, cloud file shares, and mobile devices used after hours.
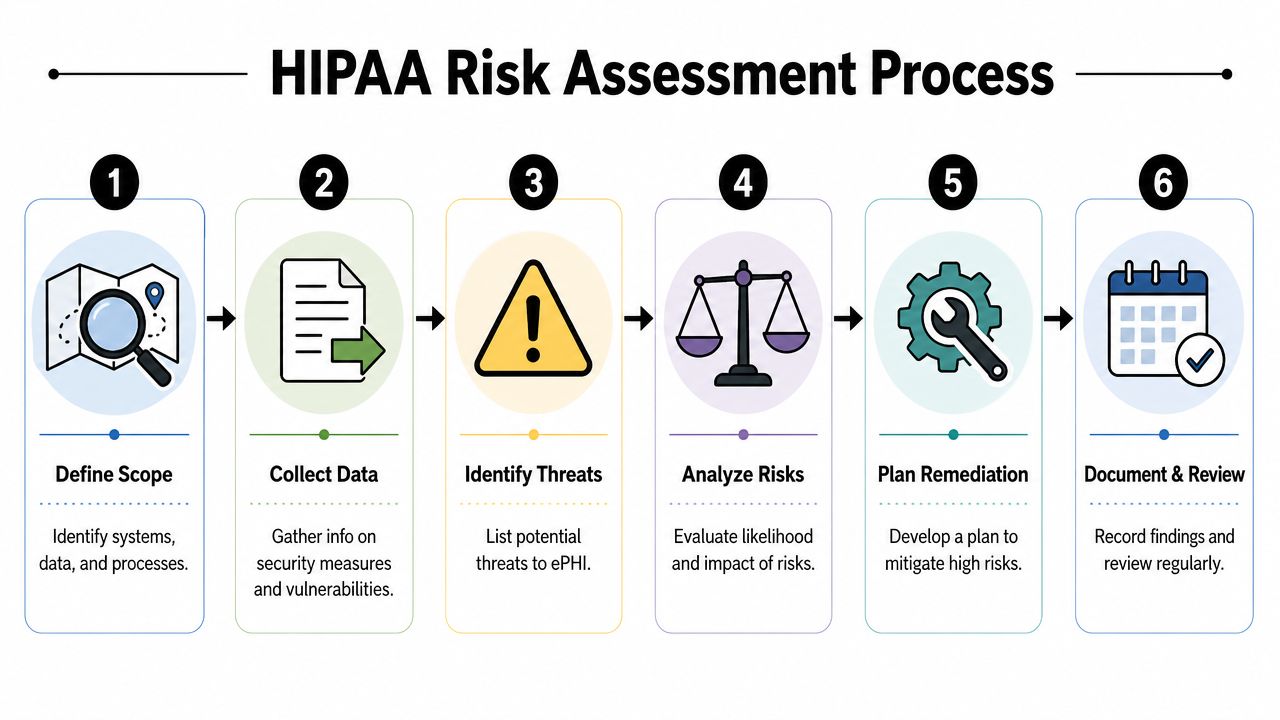
A strong assessment maps those locations first. Then it asks four practical questions:
- What data is here
- Who can access it
- What could go wrong
- What control already exists
A rigorous HIPAA risk analysis must document threats, vulnerabilities, likelihood, impact, and current controls across safeguards, with updates at least annually. It should also assign a quantitative risk level to each issue, and technical controls like Multi-Factor Authentication and encryption of PHI are required to meet Security Rule expectations, as explained in this HIPAA risk analysis guidance.
That sounds formal, but the work is practical. If staff email patient forms to themselves to print from home, that's a data flow. If terminated users still appear in old systems, that's an access risk. If a shared nurse station stays logged in all day, that's a control gap.
Score risk so decisions stop being subjective
Practices waste time when every issue feels equally urgent. They aren't.
Use a simple scoring method based on likelihood and impact. Then sort findings by what needs immediate remediation, what needs scheduled correction, and what can be monitored. That prevents leadership from spending time rewriting low-risk policy language while high-risk remote access remains weak.
A practical assessment often surfaces issues like:
- Access sprawl: Staff keep permissions long after job duties change.
- Untracked devices: Laptops and tablets aren't tied to a current inventory.
- Weak change control: New systems go live before security settings are reviewed.
- Missing evidence: Controls exist, but nobody can prove they were reviewed.
The best risk assessment produces a work list, not a trophy.
For many smaller practices, outside eyes help because internal teams normalize familiar problems. A structured HIPAA risk assessment checklist can help leadership identify what should be inventoried, scored, documented, and remediated instead of relying on guesswork.
Create Essential Policies and Manage Vendors
Policies and vendor management usually get handled by different people. That split creates blind spots. Internal behavior and outside access are part of the same risk surface.
A clinic may have decent staff rules and still create exposure through a billing service, cloud storage provider, transcription workflow, or IT contractor. That's why policy governance and vendor oversight belong in the same conversation.

Policies should control behavior, not decorate a folder
Most practices have too many unread policies and too few enforced ones. Useful policies are short, specific, and tied to daily actions.
The policy set should clearly define:
- Access use: Who may view, change, export, or send patient data.
- Device handling: How laptops, phones, removable media, and printed records are secured.
- Incident reporting: What staff report, to whom, and how quickly.
- Training expectations: What all staff complete annually and what privileged users need beyond basic training.
Annual training matters, but it isn't enough by itself. Staff need examples that match their jobs. Front-desk staff should learn scheduling and disclosure scenarios. Clinical staff should learn workstation and chart-access expectations. Managers should know escalation rules and documentation standards.
A policy earns its keep when a supervisor can use it to correct behavior the same day.
Vendors can expand risk as fast as staff can
The 2013 Omnibus Rule altered the situation by extending full HIPAA compliance obligations and direct penalty exposure to business associates and their subcontractors, closing a major liability gap, according to this summary of HIPAA business associate obligations.
That means a practice can't treat vendors like a separate issue. If a vendor handles Protected Health Information, stores it, transmits it, supports systems that contain it, or can access it during support, the relationship needs scrutiny before data flows.
A practical vendor review should answer these questions:
| Vendor question | Why it matters |
|---|---|
| Does the vendor touch PHI in any form? | Determines whether formal HIPAA controls apply |
| Is there a signed BAA before sharing data? | Prevents informal, risky onboarding |
| Who at the vendor can access systems? | Limits support sprawl and unnecessary exposure |
| How will incidents be reported? | Prevents delays during a breach investigation |
Practices that want a cleaner contract review process should understand what a strong data protection clause framework looks like before approving any technology partner.
Build Your Breach Response and Notification Plan
Every practice says it will “handle it if something happens.” That isn't a plan. A plan assigns actions, owners, timelines, and decision points before stress enters the room.
Consider a realistic event. A clinician's laptop goes missing after off-site charting. The device may contain patient information. Staff don't know whether the local files were encrypted, and the clinician used public Wi-Fi that week. Nobody should panic, but nobody should improvise either.

A calm response beats a fast messy one
The first move is containment. Disable access, revoke sessions, document the timeline, and preserve evidence. Then investigate what data was on the device, whether it was encrypted, whether remote wipe is available, and whether any access activity occurred after the loss.
After that, leadership needs a structured decision process:
- Confirm the facts: What system, what device, what data, what users.
- Assess exposure: Was PHI present and readable.
- Document the incident: Dates, actions, systems, and internal notifications.
- Determine notification obligations: Decide whether the event rises to a reportable breach.
Practices often fail because they rush to reassure everyone before the facts are known. That creates conflicting statements, poor documentation, and preventable legal complications.
During an incident, the practice needs one response lead, one evidence trail, and one approved communication path.
HIPAA breach protocols are commonly discussed in terms of investigating, analyzing, and notifying affected individuals within 60 days, but the hardest part for smaller practices is keeping the process orderly while normal patient care continues.
Insurance and notification need to be coordinated
One issue many clinics miss is the insurance side. Cybersecurity insurance has become an important operational consideration, and early contact with the insurer or broker is a worthwhile step when an incident occurs because coverage questions and claim procedures may start before the investigation is complete, as noted in this overview of HIPAA breach response considerations.
That matters because breach response isn't only technical and legal. It's financial. If a practice delays insurer notification, uses an unapproved response path, or mishandles the first phase of the event, it can create coverage problems while also trying to meet HIPAA requirements.
A written data breach response checklist for healthcare organizations helps keep that sequence disciplined when the pressure is highest.
Maintain Compliance Through Monitoring and Audits
The fastest way to weaken a compliance program is to treat it like a project with an end date. HIPAA doesn't work that way. Systems change, staff change, vendors change, and risks change with them.
That's why maintenance matters more than kickoff. A practice with decent controls and poor follow-through is less prepared than a practice with modest controls and strong review discipline.
Annual review is the floor, not the strategy
HIPAA requires covered entities and business associates to conduct annual self-audits across safeguards and to execute and annually review Business Associate Agreements before any PHI is shared, as described in this explanation of HIPAA compliance audit and BAA requirements.
Annual review is the minimum. It shouldn't be the only time anyone looks. Waiting for the calendar to force attention creates long periods where old users remain active, expired agreements stay on file, and new software enters the environment without proper review.
A practical monitoring rhythm includes:
- Monthly access review: Check privileged accounts, terminated users, and unusual access patterns.
- Quarterly vendor check: Confirm which partners touch PHI and whether agreements and contacts are current.
- Change-based review: Reassess risk after major system, workflow, or staffing changes.
- Annual formal audit: Consolidate evidence, identify gaps, and assign remediation owners.
Part-time ownership needs a real operating rhythm
Smaller practices usually struggle with this. They often don't have a full-time compliance officer, and in many cases they won't get one. That's not automatically a problem. The problem is pretending a part-time owner can manage compliance from memory.
For small clinics, especially resource-constrained practices, compliance costs can create a hard staffing cap, and part-time or shared officers are increasingly common. At the same time, requirements affecting Medicare-certified Rural Health Clinics are tightening, including officer designation expectations discussed in this overview of HIPAA compliance for rural health clinics.
The workable model is operational, not heroic:
- Use recurring calendar blocks: Compliance work needs protected time.
- Use a tracked system: Tasks, evidence, reviews, and open issues should live in one place.
- Assign backups: One person shouldn't hold all procedural knowledge.
- Review drift early: Shared officers need a routine to catch overdue tasks before they pile up.
A managed partner can make this sustainable by handling monitoring, patching, log review support, and security operations in the background while the practice maintains ownership of decisions. That's often the most efficient path for a busy healthcare office that needs reliable HIPAA compliance for healthcare without building a full in-house compliance department.
Frequently Asked Questions About HIPAA Compliance
Does a small practice need a full-time HIPAA officer
Not always. Small and mid-sized practices often rely on part-time or shared ownership. What matters is documented responsibility, scheduled oversight, and evidence that tasks are completed.
How often should staff be trained
Staff should receive annual HIPAA training, and privileged users need role-based training beyond the general material. Training should be tied to real scenarios, not generic slides.
Are cloud tools automatically HIPAA compliant
No. A practice should verify whether the vendor handles PHI, whether access is appropriate for the minimum necessary rule, and whether a Business Associate Agreement is in place before any PHI is shared.
What's the biggest compliance mistake
Treating compliance like a document exercise. Most failures come from weak execution, stale reviews, human error, and unmonitored vendor relationships.
When should a practice review BAAs
Before any PHI is shared, then annually, and again whenever the relationship, service scope, or access pattern changes.
A healthcare practice doesn't need more generic advice. It needs a compliance system that works effectively, especially when leadership is busy and internal bandwidth is limited. Technovation LLC helps North Texas organizations build that system through cybersecurity support, compliance readiness, proactive monitoring, IT health checks, and practical guidance that fits daily operations. For practices that want a clearer path to resilient HIPAA compliance for healthcare, Technovation is a smart next call.






